



Kindlmann G, Ennis DB, Whitaker RT, Westin CF. Diffusion tensor analysis with invariant gradients and rotation tangents. IEEE Trans Med Imaging. 2007;26(11):1483–99.
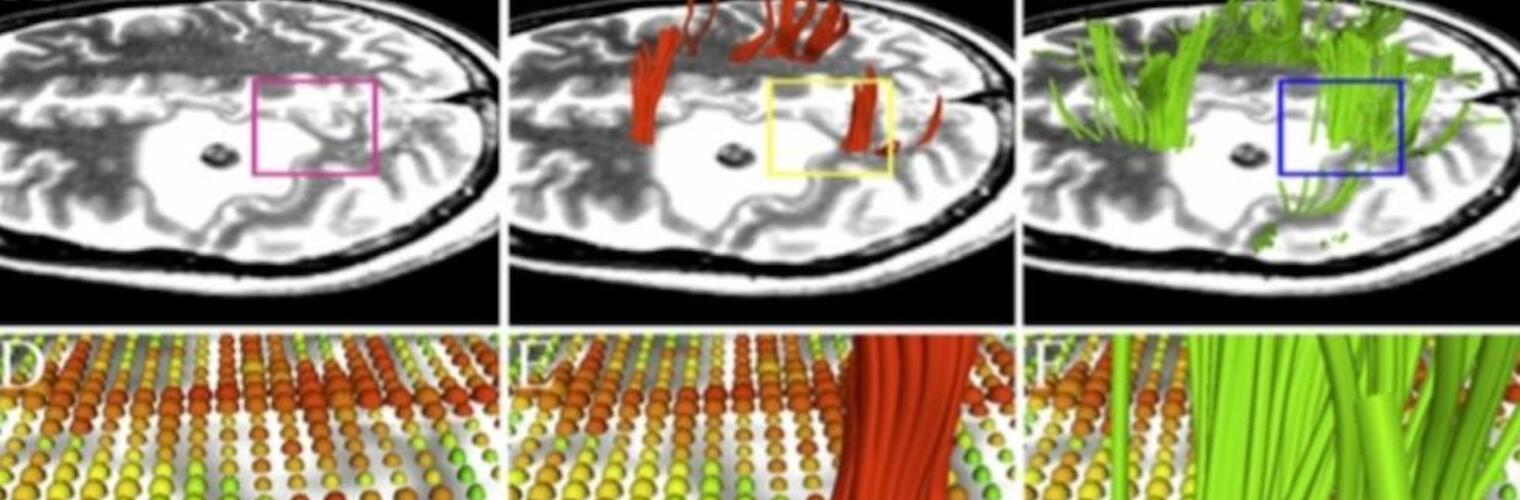
Guided by empirically established connections between clinically important tissue properties and diffusion tensor parameters, we introduce a framework for decomposing variations in diffusion tensors into changes in shape and orientation. Tensor shape and orientation both have three degrees-of-freedom, spanned by invariant gradients and rotation tangents, respectively. As an initial demonstration of the framework, we create a tunable measure of tensor difference that can selectively respond to shape and orientation. Second, to analyze the spatial gradient in a tensor volume (a third-order tensor), our framework generates edge strength measures that can discriminate between different neuroanatomical boundaries, as well as creating a novel detector of white matter tracts that are adjacent yet distinctly oriented. Finally, we apply the framework to decompose the fourth-order diffusion covariance tensor into individual and aggregate measures of shape and orientation covariance, including a direct approximation for the variance of tensor invariants such as fractional anisotropy.