



Ferrant M, Nabavi A, Macq B, Black PM, Jolesz FA, Kikinis R, Warfield SK. Serial registration of intraoperative MR images of the brain. Med Image Anal. 2002;6(4):337–59.
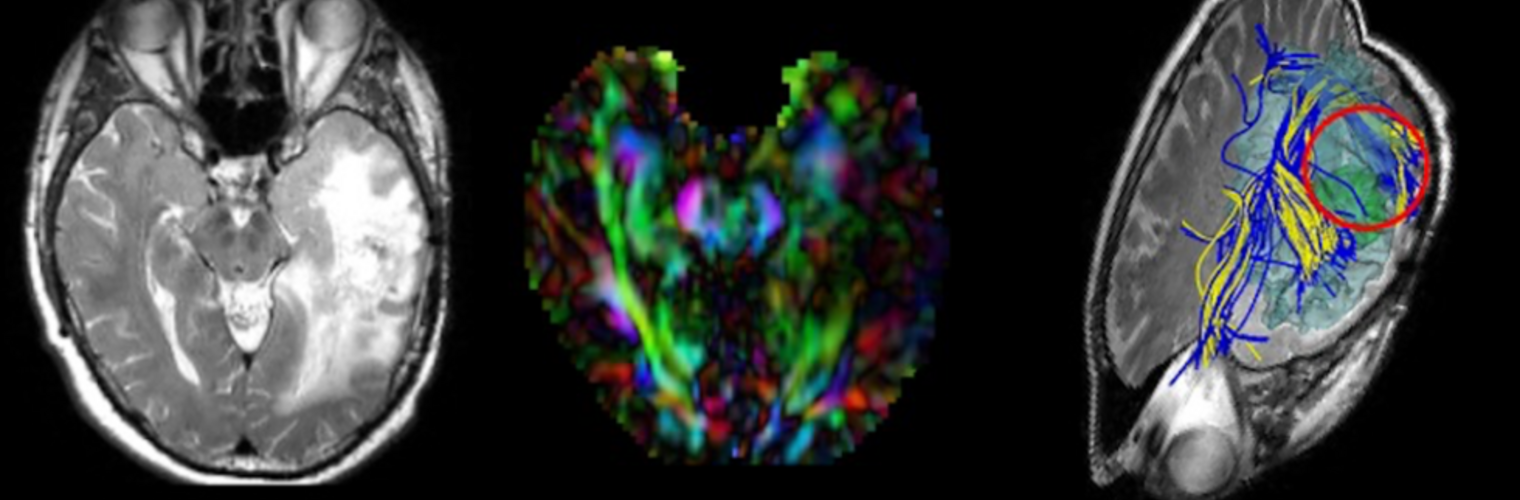
The increased use of image-guided surgery systems during neurosurgery has brought to prominence the inaccuracies of conventional intraoperative navigation systems caused by shape changes such as those due to brain shift. We propose a method to track the deformation of the brain and update preoperative images using intraoperative MR images acquired at different crucial time points during surgery. We use a deformable surface matching algorithm to capture the deformation of boundaries of key structures (cortical surface, ventricles and tumor) throughout the neurosurgical procedure, and a linear finite element elastic model to infer a volumetric deformation. The boundary data are extracted from intraoperative MR images using a real-time intraoperative segmentation algorithm. The algorithm has been applied to a sequence of intraoperative MR images of the brain exhibiting brain shift and tumor resection. Our results characterize the brain shift after opening of the dura and at the different stages of tumor resection, and brain swelling afterwards. Analysis of the average deformation capture was assessed by comparing landmarks identified manually and the results indicate an accuracy of 0.7+/-0.6 mm (mean+/-S.D.) for boundary surface landmarks, of 0.9+/-0.6 mm for landmarks inside the boundary surfaces, and 1.6+/-0.9 mm for landmarks in the vicinity of the tumor.